


C19 incidence - the most useless time series
Billions for knick-knacks

At least in Germany the C19 case incidences showed extreme fluctuations over the last nearly 4 years. The test regimes were changed several times, possibly explaining the massive distortions. For a while, this view seemed prevail among experts. Recently, however, some argued again based on such observations. In the following statistical analyses, I will provide insights proving as well as challenging several arguments.
No PCR tests were broadly available during the very first phase of the C19 pandemic, so no data is available on this. Meanwhile we known from wastewater samples and blood donations that C19 was already circulating in Europe in fall 2019. This was followed by a phase in which PCR tests were in short supply. Here an underestimation of infections can be assumed also. Later, when plenty of tests were available, the test numbers gradually rose to higher levels. This increased even further after rapid antigen tests became mandatory in schools and other institutions. As a result, more infected people were identified than before. The threshold of the CT value in the PCR test, which indicates a positive test result, varied as well as several other details in laboratory diagnostic. In the healthcare sector, high premiums were paid for C19 patients during certain periods, which created a huge incentive to stop looking for other diseases if a positive result was found. Differential diagnoses were often no longer carried out in these cases. The logical consequence was a mass relabeling of all possible diagnoses as C19 cases and C19 deaths.
So far for the background. Now let's test some time series. These are the all-cause deaths, excess mortality (raw data source: Destatis) and the C19 cases and C19 deaths in Germany (source: Johns Hopkins). Due to availabilty, the data series last from calendar week 4 in 2020 to calendar week 10 in 2023 as plottet in Fig. 1.
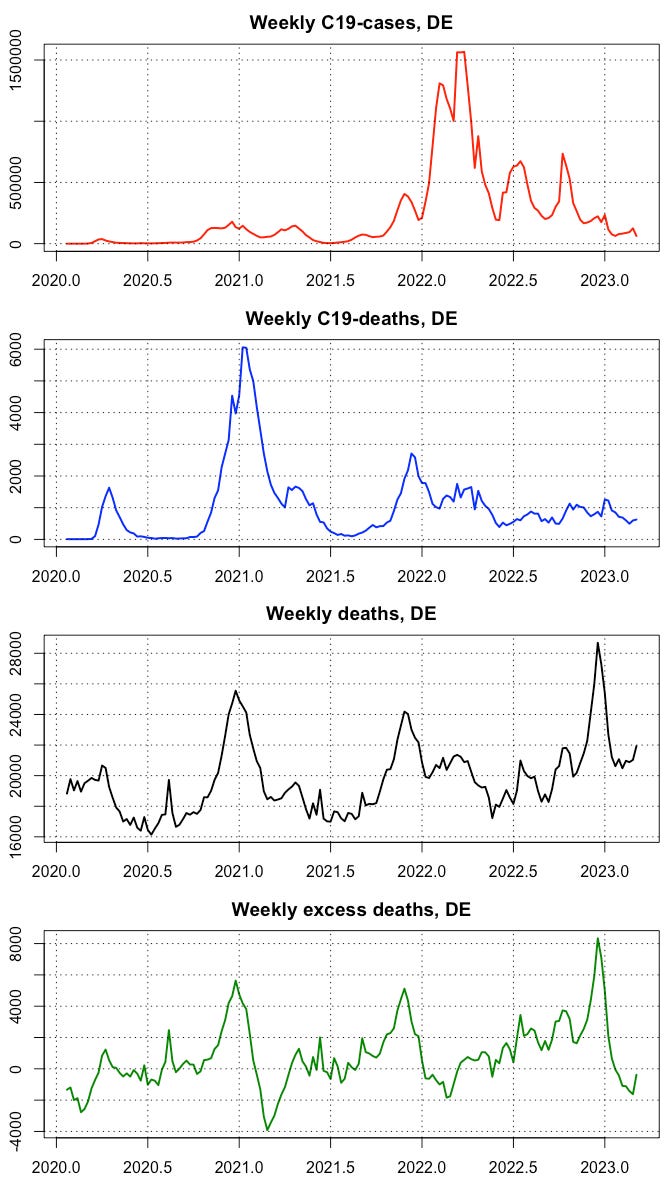
Fig. 1: Time Series of C19 cases (pos. PCR test), C19 deaths, all cause deaths and excess mortality. The excess mortality was obtained from the weekly risks in 14 age cohorts, for which trend and saisonality were determined separately during the reference epoch 2012-2020 to create expected values for the later weeks and calculate the difference to the reported cohort deaths. These cohort differences are finally added up to one number for each week.
Let’s watch the correlations (Tab. 1).

Tab. 1: Correlations and p-values in brackets. Significant correlations are shown in bold.
1st result: C19 cases and C19 deaths show only a poor, non-significant correlation. (top left)
2nd result: C19 cases and excess deaths show a nearly Zero correlation, non-signifikant. (bottom left)
It can therefore be said that there was no correlation at all between the C19 case numbers and the only relevant variable, excess mortality.
High and significant correlations also exist. The connection between all-cause deaths and excess deaths is logical and self-evident. I only mention it for the sake of completeness.
3rd result: We get a high-significant correlation of C19 deaths and all cause deaths (mid). However, this is weakened if the C19 deaths are put in relation to the excess deaths (bottom mid). This possible contradiction may be explained by the fact that all-cause deaths have a saisonal pattern, which is largely eliminated with the variable excess-death.
4th result: C19 cases seem to correlate with all-cause deaths, but this vanishes, if we replace the latter by the excess deaths. Same explanation as above.
How are positive correlations possible if the C19 cases are not related to either C19 deaths or excess deaths? A plausible explanation is that a high proportion of normal deaths could have been relabeled as C19 deaths. The strong connections with the all-cause deaths result from temporal relationships with the seasonal wave, and it weakens when one moves on to the excess deaths. However, the excess deaths also contain residual seasonal components, so that the connection to the C19 deaths does not vanish completely. It was even to be expected that a residual connection would remain, because one can undoubtedly die from C19. However, not to the extent that the incidence figures seem to tell us.
The results regarding the C19 cases can be evaluated with a Granger causality test for further validation. Granger causality means, the knowledge of A at a given time is useful to predict B later. This is exactly the scenario, if poeple get an infection (C19 cases) and die from it some days later. I applied the test with a lag of max 3 weeks (Tab. 2).

Tab. 2: Granger causality test. If p > 0.05, the Null-hypothesis H0 that there is no Granger causality has to be rejected.
We recognize that the C19 cases cannot be considered causal neither for the C19 deaths nor for the all-cause deaths, since the p-values are well above 0.05. There was also no connection with the excess deaths, as the above correlation calculation has already shown.
But the same tests in reverse direction reveals a causality, as if for unknown reasons C19 deaths led to more C19 cases. OK, some funny oddities are part of the business, especially when you're examining such dubious variables as C19 incidence. That's exactly what this study shows. They are highly distorted and are good for nothing. Billions were spent collecting these figures, and they provided the bogus justification for cruel restrictions on civil rights.
I would like to see the correlation of C19 cases, shifted 1, 2, 3, o 4 weeks backwards, and C19 death, ACD and excess deaths.
The same, if possible, for same large countries, such as England or UK, France, Italy, Spain.
I would be interested to see if there was any correlation between PCR test-positivity rates and Covid deaths or all-cause deaths?